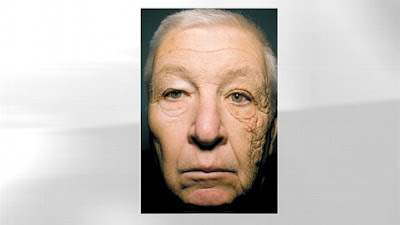
Historically differentiation between male and female skulls was performed by anthropologists and medical examiners by analyzing nose, chin and forehead bone shapes in cadavers. Today it is common knowledge that faces contain secondary sex characteristics that develop during puberty and make male faces easily distinguishable from female faces. The female chin is more rounded or pointed than the square male chin and their less prominent noses have less angular tips . The male forehead has a prominence of bone, a horizontal ridge of bone, running across the forehead just above the eyebrows (bossing), followed by a concave area and then slopes upward and backward. The female forehead lacks bossing and the concave area above it and rises vertically rather than sloping upward and backward.
Additionally as is evident in these photos the angle of the lower jaw in front of and below the ears is more prominent in males
Facial feminization surgery (FFS) is a set of surgical procedures, first described in the late 1980s, that alter typically male facial features to make them closer in shape and size to typical female facial features. Facial feminization surgery includes various bone and/or soft tissue procedures such as foreheadplasty to change the shape of the forehead bone or move the frontal hairline, brow lift, rhinoplasty, cheek implantation, and lip augmentation as well as facial hair removal. FFS is medically necessary to treat gender dysphoria. It can be as or more important than genital forms of sex reassignment surgery to these patients thereby allowing them to integrate socially as women. Studies have shown that the mental health-related quality of life for trans women who have had FFS is significantly higher than for trans women who have not had FFS. Non-transsexual women who feel that their face is too masculine or simply want to improve their looks can also benefit from some of these procedures.
HAIRLINE CORRECTION BY SCALP ADVANCEMENT- HAIRGRAFTING - BROWLIFTING In males the hairline is often higher than in females and usually has receded corners above the temples that give the hairline an “M” or "V" shape. Females have lower corners at the temples and are higher in the midline (an inverted U-shape). The hairline can be moved forwards and given a more rounded shape either with a procedure called a “scalp advance” where the scalp is lifted and repositioned or with hair transplantation. Hair transplants can also be used to thicken up hair that has been thinned by male pattern baldness. If too much hair has been lost, it will obviously not be possible to correct hairline problems.
Before and After Scalp AdvancementNote the vertical orientation of this female forehead without forehead bossing. In genetic males feminization of the hairline requires advancement and reshaping to this pattern. Advancement alone is not sufficient and some patients only need advancement of the corners at the temples for feminization. The shape of the hairline is more important than the height! In performing the advancement inked needles are passed through the skin to mark the current and desired hairline level on the bone. An incision is made at the hairline and the scalp lifted up all the way to the back of the skull as needed. Relaxing incisions on the sides of the scalp an under it allow the scalp to come forward to the marked level on the bone, excess forehead skin is removed and the scalp is suture quilted to the skull to prevent later retraction of the scalp and over elevation of the eyebrows. This procedure is contraindicated in smokers due to the risk of loss of scalp tissue in such patients.
There is always a visible scar from a scalp advance but just how visible will be partly down to luck, partly down to the skill of the surgeon and partly down to your own tendency to scar. Many patients feel their scar is almost invisible except to people who know what they are looking for. The scalp advance technique severs two nerves that supply sensation to the scalp. The sensation often does not fully return and you may notice one or two numb or partially numb patches on your scalp. This is not generally a problem though and you only tend to notice the numbness if you are feeling for it. The hair growing near the incision may fall out after a scalp advance. This hair will start to grow again 3 to 4 months later
Since female eyebrows are typically higher than male eyebrows the advancement is designed to create a browlift at the same time when necessary. Doing so when it is not necessary will leave you with eyebrows in an unnaturally high position and an unusual "surprised" expression. In such cases the scalp advancement can be performed without a browlift.
FOREHEAD RECONTOURING Changing the shape of the skull in the forehead area (foreheadplasty) changes one feature from distinctly male (bossing and backward sloping) to distinctly female (vertical without bossing).
The forehead bone can be one of 3 types:
- The bone of the bossing is thick and the frontal sinus deep to it is small or absent and the bossing may appear greater than it actually is due to a deep concave or indented area just above it
- The bossing is present but the bone is thin and the frontal sinus may be large i.e. the bone is too thin to burr down
- The sinus is so large and protrudes so far forward that the bone cannot be burred or filed down without entering the sinus
The first is treated by burring with or without methylmethacrylate (shave and fill), the second with only methylmethacrylate placed to fill in the indented areas and the third by cutting the bone setting it backward, burring/reshaping as necessary and fixing it in position with wires or plates and screws. Absorbable plates and screws dissolve within 6 to 12 months. If the bone is cut, reshaped and fixed in place an overnight stay in an aftercare facility is prudent. Some patients have a tissue reaction to methylmethacrylate and secrete fluid around it for a week or two after surgery. This is removed with a syringe and needle until the body no longer produces it. Hydroxyapatite bone cement, commercially available as BoneSource, can be used instead of methylmethacrylate to smooth out any visible step between any bossing present after burring and the rest of the forehead to provider a smoother surface with a more vertical orientation for a more feminine appearance. All of these procedures can be performed via the same incision used for scalp advancement.
![]()
![]()
This is a case where the bone was cut out flattened and then placed back in position by
Dr. Barry Eppley. This is a case of forehead reshaping without feminization because the backward upward slope of a male forehead was maintained.
RHINOPLASTYMen have triangular shaped noses with wider bases near the upper lip and more downwardly displaced nasal tips than women. Female noses have a more concave contour along the sidewalls that flows smoothly downward from the inner end of the eyebrows. Standard rhinoplasty procedures are generally suffice to successfully feminize a nose. Rhinoplasty is effective in achieving female facial profiles in patients undergoing male-to-female sex reassignment.
These photos show the more triangular shaped male nose with a wider base compared to the concave sidewalls and narrower base of the female nose. Also note the higher eyebrows in the female and the more squared chin contour in the male.
![asian rhinoplasty]()
![asian rhinoplasty]() Feminization of the nose by making the sidewalls concave, raising the tip and narrowing the base in genetic females.CHEEK IMPLANTS
Feminization of the nose by making the sidewalls concave, raising the tip and narrowing the base in genetic females.CHEEK IMPLANTSFemales often have more forward projection in their cheekbones as well as fuller cheeks overall. The fleshy part or “apple” of female cheeks contains more fat than the male and is therefore fuller and rounder – male cheeks are much more hollow here. The hormones taken by transsexual patients can increase the fat here but it may take a year of hormone therapy for this to occur so it is best to wait a year before doing cheek surgery. If this is insufficient free fat graft injections using fat liposuctioned from elsewhere on the body and/or shifting soft tissue at the time of facelift surgery can do the job. (
See My Blog on Free Fat Grafting) Sometimes cheek implants are used to feminize cheeks. They come in different sizes and can be placed in different positions depending on the needs of the patient. Sometimes bone cement (hydroxyapatite cement) is used instead of silicone implants but various other materials such as goretex or porous polyethylene are also used.
These medpor cheek implants were placed via an incision inside the mouth.
CHIN IMPLANTS OR RECONTOURINGMales tend to have taller chins than females with a deeper labiomental fold between the lower lip and chin. Female chins tend to be rounded and male chins tend to be square with a flat base and two corners. The chin can be reduced in height either by bone shaving or with a procedure called a “sliding genioplasty” where a section of bone is removed. The square corners can usually be shaved down. In other cases placement of a small round chin implant will suffice. Fat injection into the labiomental fold is a nice easy way to feminize the chin for those with deep labiomental folds. Sometimes liposuction is also used to remove some of the fat that some people have underneath the chin although that is more to improve looks than feminize the face. It is also a very good source of fat for the labiomental fold.
LIP AUGMENTATIONThe distance between the opening of the mouth and the base of the nose tends to be longer in males than in females and in older individuals vs. younger individuals. When a female mouth is open and relaxed the upper incisors are often exposed by a few millimeters. Feminization has been performed by making an incision just under the base of the nose to remove a section of skin,"subnasal lift". or removing a segment of skin just above the upper lip along its entire length,"vermilion advancement". I personally did not do either of these because of their potential for visible uncontrollable scarring. I prefer lip augmentation with fat injection or Alloderm and elevation during the process of a subperiosteal facelift. Neither of these approaches creates a visible skin scar between the nose and upper lip.
Lip augmentation using Alloderm to give a feminine pouty look..
Injectable fillers like Juvederm, Restylene etc are regularly used to augment lips but are not my preferred method because they do not last long.
LIPOSUCTIONLiposuction is more for improving looks than feminizing per se but can be used to masuclinize the face if performed to emphasize the jaw line or to harvest fat for feminizing fat injections.
JAW RESHAPINGMales’ jaws tend to be wider and taller than female jaws and often have a sharp corner at the back. The back corner can be rounded off in a procedure called “mandibular angle reduction”; bone can also be shaved off along the lower edge of the jaw to reduce width and height and the chewing muscles (masseter muscles) can also be reduced to make the jaw appear narrower. The angle reduction is performed via an incision inside the mouth using an x-ray template to prevent removing too much bone. Pressure dressing and a head up position are required to decrease swelling. An overnight stay in an aftercare facility is prudent to ensure that swelling is well controlled and that you can take food orally after surgery.
TRACHEAL SHAVING-ADAM'S APPLE REDUCTIONMales tend to have a much more prominent Adam's apple than females although small Adam's apples are more common in males than many people realise. The Adam's apple can be reduced with a procedure called a “tracheal shave” or “Chondrolaryngoplasty”. This is best done via an incision in the natural neck skin crease above the Adam's apple to give the least noticeable scar. It is not always possible to make a large Adam’s apple invisible with this procedure, rather the intent is to change it from the masculine 90 degree Adam's apple angle to the feminine 120 degree Adam's apple angle.
![]()
![]()
The voice is temporarily weakened by this procedure and the weakened state can last for as long as 6 months but permanent changes to the voice are possible. The cartilage that forms the Adam’s apple tends to harden with age and that may limit the amount that can be removed in an older patient. There is also a limit to how much can be removed without risking permanent damage to the voice. Basically, the Adam's apple is part of the front wall of the voice box and the vocal chords are attached to that wall - if the wall is thinned too much, it may no longer be strong enough to hold the vocal chords in full tension. This can leave the voice deeper and with a gravelly sound.
LASER HAIR REMOVAL OR ELECTROLYSIS OF THE BEARDBeautification and rejuvenation procedures are often performed at the same time as facial feminization. For example, it is common for eye bags and sagging eyelids to be corrected with a procedure called “blepharoplasty” and many feminization patients undergo a face and neck lift (rhytidectomy). Along with scalp advancement/forehead recontouring the muscles creating frown lines between the eyebrows can be removed and the frown lines can be filled with grafts. It is often necessary for older patients to have a lower face-lift after jaw and chin surgery because the reduction in bone and the effects of swelling can leave sagging skin. Nasolabial folds between the nose and corners of the mouth can be diminished with filler injections. FFS is a very powerful set of procedures but there are limits; for example: a wide jaw can be feminized by surgical narrowing but it may not be physically possible to narrow a very wide jaw enough to make it fully female. There are also some masculine facial features that can't be surgically feminized at all like the relative size of the eyes to the skull (females tend to have proportionately larger eyes).
Facial proportions analysis in cosmetic surgeryAaron Stone MD - Plastic Surgeon Los AngelesDr. Stone's Twitter
![Medicine Blogs - BlogCatalog Blog Directory]()
![]()
![Listed in LS Blogs the Blog Directory and Blog Search Engine]()
![]()
![Add to Technorati Favorites]()
![blog search directory]()
![]()
![Health Blogs - Blog Rankings]()

![Blog-Watch - The Blog Directory]()
![Webfeed (RSS/ATOM/RDF) submitted to http://www.feeds4all.nl]()